
We will talk about THORACIC OUTLET SYNDROME, one of the prevalent syndromes, in today’s article. As the title suggests, we will study this syndrome, its etiology, clinical manifestations, and treatment options, in addition to the thoracic outlet syndrome exercises. But first, let’s examine the thoracic outlet and its structure in order to fully comprehend this disease.
ANATOMY OF THORACIC OUTLET
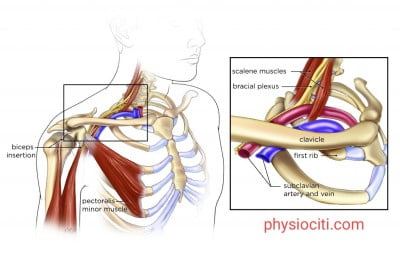
The area between the clavicle, the scalene muscle, and the first rib is known as a thoracic outlet. Located in the lower neck region, directly above and beyond the clavicle, is the thoracic outlet.
The brachial plexus, axillary artery and vein, and subclavian artery and vein are among the neurovascular bundles found in the thoracic outlet.
WHAT IS THORACIC OUTLET SYNDROME (TOS)?
Compression of the neurovascular bundles that include the brachial plexus, axillary artery and vein, and subclavian artery and vein at the thoracic outlet results in thoracic outlet syndrome (TOS).
When this area narrows, either because of hypertrophy of the current muscles or because of other factors like congenital, trauma, etc., the structures mentioned above run the risk of being crushed. When the space at the thoracic outlet or inlet is insufficient, the neurovascular systems put undue strain on their entry into the upper limbs through this area.
SITES OF COMPRESSION
Compression can occur at the supraclavicular, subclavicular, or infraclavicular locations.
- SUPRACLAVICULAR: At the inter scalene triangle between the anterior scalene muscles.
- SUBCLAVICULAR: At the interval between the 2nd thoracic rib, clavicle, and subclavius.
- INFRACLAVICULAR: Beneath the enclosure formed by the coracoid process, pectoralis minor, and costocoracoid membrane.
- RARE CAUSES: Scissor-like encirclement of the axillary artery by the median nerve.
CONTRIBUTING FACTORS
DYNAMIC FACTORS
Full abduction of the arm draws the artery up 180 degrees, potentially compressing the short retroclavicular region.
STATIC FACTORS
- Vigorous occupation increases the muscle bulk and thereby decreases the space.
- Inactive occupation decreases the muscle bulk and thereby increases the space.
- Arteriosclerosis
- Anomalies of the first thoracic rib
- Malunion or nonunion of the fracture clavicle.
- Congenital cervical rib decreases the inter scalene space and thereby decreases the retro clavicular space.
- Miscellaneous-
- Tumors arising from the upper lobe of the lung
- Cervicothoracic scoliosis
- Abnormal variations of the scalene muscles
CLINICAL FEATURES
This syndrome poses two main problems. The first one relates to the compression of major vessels and the second to the compression of nerves.
VASCULAR PROBLEMS:
Venous or arterial compression may be the cause of vascular issues.
The patient has quick weariness during overhead tasks and complaints of numbness over their entire arm during the early stages of moderate artery compression. In the event of substantial compression, the patient may experience pallor, cyanosis, and cold, and Raynaud’s phenomenon.
Following activity, the leg will be swollen and discolored due to venous compression; these symptoms will gradually go away with rest.
NEUROGENIC PROBLEMS:
This involves the C8 T1 segment (Klumpke’s paralysis). The patient will report having paraesthesia in the little, ring, and arm medial aspects. Additionally, there is a hand weakness.
COMPLICATIONS OF TOS
Compression of the subclavian artery causes post-stenotic dilatation, which in turn causes statis to favor thrombosis. The thrombi then rupture and migrate distally, causing embolization, which in turn causes distal arterial blockage, which in turn causes ischemia and gangrene in the upper limbs.
INVESTIGATIONS
- X-Ray neck- To rule out intrinsic causes like cervical spondylosis, cervical rib, etc.
- Nerve conduction studies- Difficult to determine the nerve conduction studies through the thoracic outlet, but its biggest value is to rule out problems like entrapment, e.g., the ulnar nerve at the elbow, wrist, etc.
TREATMENT
- CONSERVATIVE TREATMENT- It consists of rest and pain killers.
- SURGICAL TREATMENT- It is indicated in gangrene and post-stenotic dilatation.
- Methods:
- Removal of first thoracic rib- This is the most effective treatment as it deals with both supraclavicular and infraclavicular factors.
- Removal of cervical rib- If this is the cause of the compression.
- Scalenotomy- It is indicated in scalenus anticus syndrome.
- Methods:
PHYSIOTHERAPY MEASURES
- THERMOTHERAPY- For pain relief and relaxation.
- Manipulate and mobilise and relax 1st rib and clavicular, scapular, pectoral muscles.
- STRENGTHENING EXERCISES– Strengthen the shoulder girdle muscles and stretch scalene muscles.
- RESTORATION OF NORMAL POSTURE– Proper postural changes and correct faulty postures.

THORACIC OUTLET SYNDROME EXERCISES
Thoracic Outlet Syndrome Exercises:
- Look straight ahead while sitting or standing.
- Bend your right ear towards your right shoulder.
- Hold the stretch for 20 sec.
- Repeat with the other side as well.
- Do it 10 times each side twice a day.

- Begin in a quadruped position ( Both legs and hands on the ground).
- Raise one hand to the sky and keep the other hand steady while you open your chest to the sky.
- Get back your hand to the starting position and do this 10 times.
- Repeat with the other side as well.
- Try to maintain a neutral spine and do controlled and slow movements.

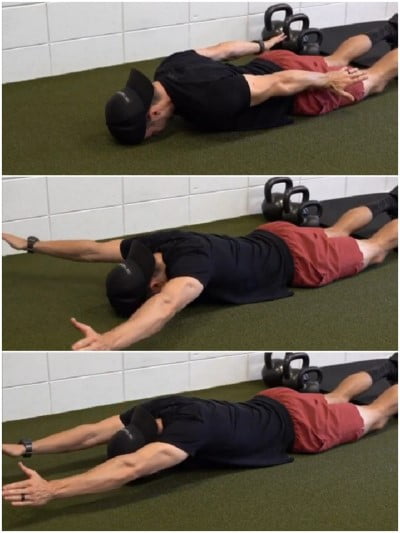
- Place yourself on your back or side, or in a prone position.
- Stretch your arms and both legs out.
- Make a wide, controlled arc with your hands, palms facing the floor, starting at your hips and ending at the top of your head.
- Elbow should remain in extension position throughout the movement.
- Chin stays tucked and abs engaged to avoid arching of the back.
- Repeat this movement 10 times.
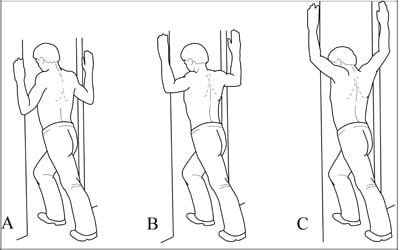
- Start with your elbows low.
- Lean your body weight forward until you feel a stretch in front of your shoulder or chest.
- Now do the same with elbows at shoulder height and then slightly more towards the ceiling.
- Do this stretch 5 times with each position.
NOTE: Do not overstretch your muscles.
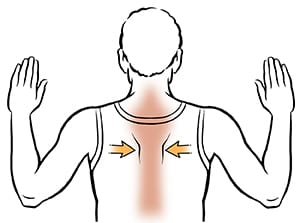
- Bend your elbows as you raise your arms to shoulder height.
- Your palms should face forward.
- Squeeze both your shoulder blades together and hold for 10 seconds.
- Do it 10 times.
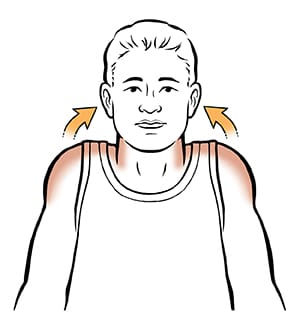
- Stand straight by your hands to the sides of your body.
- Your palms should face your body.
- Now shrug your both shoulders.
- Repeat for 10 times.
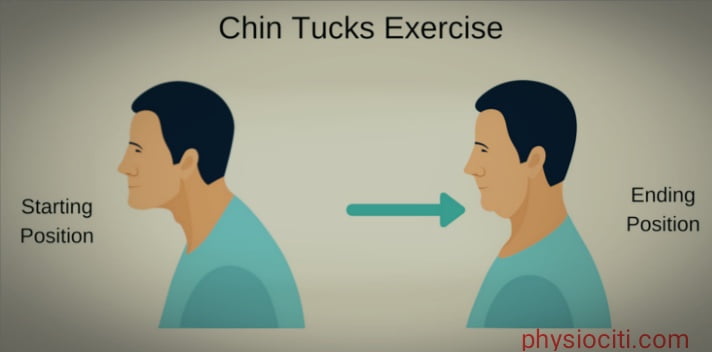
- Pull your chin back as you are making a double chin.
- Hold for 5-10 seconds and then relax,
- Repeat 10 times.
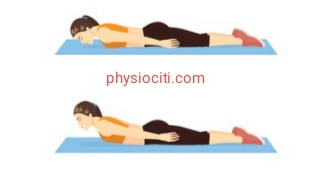
- Lie down on your abdomen.
- Put your hands on your sides.
- Lift your head as well as your chest off the floor.
- Hold for 5 seconds and then relax.
- Repeat 5-10 times.

CONCLUSION:
Thoracic outlet syndrome (TOS) is a common yet difficult condition that we have examined in today’s article. Its clinical characteristics, etiology, consequences, and course of treatment have all been covered. Exercises for thoracic syndrome, as previously indicated, can be quite beneficial in treating this illness.
Note that you should never exercise without first consulting your physiotherapist.
ALL THE BEST!