
Frozen shoulder or Periarthritis or Adhesive capsulitis is a clinical syndrome where there is a painful restriction of both active as well as passive shoulder movements. The shoulder joint is the most mobile joint and this mobility makes it very vulnerable to problems that ultimately “freeze” its movements. Today, in this article we are going to discuss frozen shoulder exercises, their causes, and physiotherapy treatment.
Causes:
The causes are mainly idiopathic and are due to fibrosis followed by chronic inflammation. This could be due to:
Primary shoulder causes
Problems directly related to the shoulder joint which can give rise to a frozen shoulder are tendinitis of the rotator cuff, bicipital tendonitis, fracture, and dislocations around the shoulder.
Secondary non-shoulder causes
Problems not related to shoulder joint like diabetes, hyperthyroidism, hypertriglyceridemia, cardiovascular diseases with referred pain to the shoulder which keeps the shoulder immobile, reflex sympathetic dystrophy, frozen hand shoulder syndrome, a complication of colles’ fracture can all lead to frozen shoulder. The reason can be immobilization of the shoulder joint for a longer period of time due to referred pain etc.
Pathogenesis:
- During abduction, repeated overhead activities of the shoulder, long head of biceps, and rotator cuff undergo repeated strain. This results in inflammation, fibrosis, and thickening of the shoulder capsule. It results in loss of movement. If the movements continue, then the fibrosis gradually breaks, and movements return but never come back to normal.
- Prolonged activity causes small scapular and biceps muscles to waste faster, load on joint increases, and degenerative changes set in. There is fibrosis of the capsule and a decrease in shoulder movements.
Clinical Features:
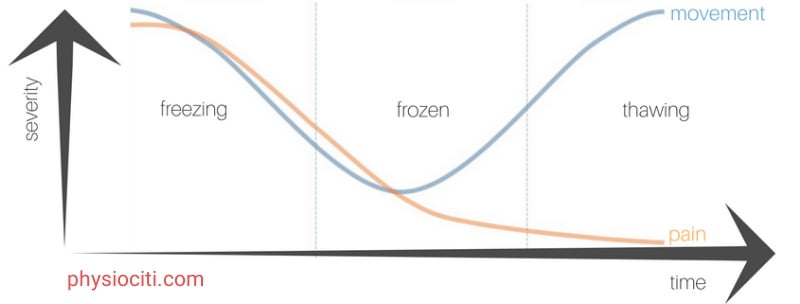
There are 3 stages in the frozen shoulder:
STAGE 1: (STAGE OF PAIN/FREEZING)
The patient complains of pain with insidious onset, decreased movements, external rotation greatest followed by loss of abduction and then forward flexion. Effect on internal rotation is least. This stage lasts for 10 to 36 weeks. Pain due to frozen shoulder is mainly nocturnal and usually doesn’t radiate below the elbow.
STAGE 2: (STAGE OF STIFFNESS/FROZEN)
In this stage, the pain gradually decreases and the patient complains of a progressive stiff shoulder in a capsular form. Slight movements are present.
STAGE 3: (STAGE OF RECOVERY/THAWING)
The patient will have no pain and movements will recover but will never come to normal. It lasts for 6 months to 2 years. The effect on ADL is severe.
Treatment:
STAGE 1:
In this stage, long-acting once-a-day NSAIDs are usually helpful as this condition usually runs a long course (10-36 weeks). Intra-articular steroids may also help. Thermotherapy using TENS or alternative therapies like acupuncture also helps in this stage.
STAGES 2 & 3:
A stiff shoulder is a challenge to the physiotherapist and the patient alike since it thwarts the best attempts to restore back the earlier free shoulder movements. A ‘sustained approach’ rather than an ‘aggressive approach is the ‘mantra’ in these patients.
The ‘twin approach’ needed to put the shoulder joint back on its rails is shoulder mobilization as well as strengthening of the muscles.
Shoulder Mobilization Techniques:
The real culprit for the shoulder stiffness is the thick and contracted capsule of the shoulder joint. Efforts should be done for softening this capsule by passive mobilization.
ROLE OF THE PHYSIOTHERAPIST
The physiotherapist can use the following options to achieve his goals:
- THERMOTHERAPY
Before restoring to passive mobilization, the thick and contracted capsule can be relaxed and made more stretchable by deep heating using ultrasonic or other suitable modalities as well. The heating is carried out all around the shoulder with a special focus on the anteroinferior border of the axilla where the basic defect is said to exist.
- PASSIVE MOBILIZATION TECHNIQUES
After the thermotherapy, a physiotherapist should observe the following protocol for passive mobilization of the shoulder joint.
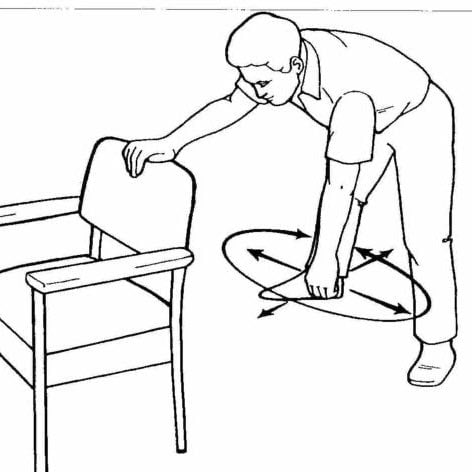
In the forward stoop position
In this position, the physiotherapist stabilizes the shoulder joint with his one hand and grasps the wrist with the other hand. Then a slow rhythmic circumduction movement is carried out up to the limit of pain.

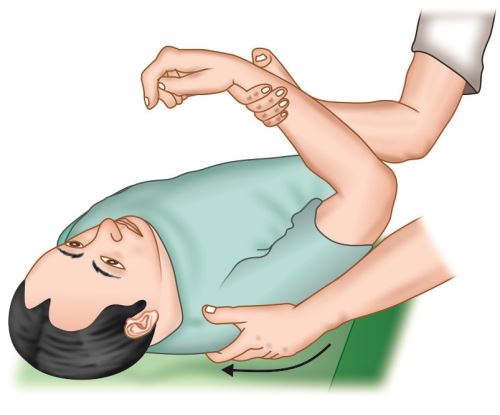
In the supine position
Here the patient is supine and the shoulder is in a position of maximum abduction, neutral rotation with the elbow in 90 degrees of flexion. The physiotherapist now grasps the arm with his hand and will then apply longitudinal traction along the axis of the humerus, he carries out an anterior-posterior glide and an abduction-adduction glide also in a slow rhythmic manner.
Both the above passive mobilization techniques are very effective in mobilizing the stiff shoulder.
ROLE OF THE PATIENT
In the physiotherapy treatment for frozen shoulder, this is the most important method of the patient healing himself by a ‘home-treatment’ regimen. These frozen shoulder exercises should be performed by the patient at home as well as at the clinic.
Frozen Shoulder Exercises:
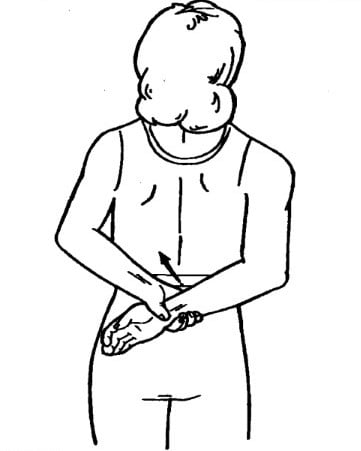
In a forward stooping position, with one hand resting on a chair, the patient swings his arm like a pendulum and then carries out a circular movement.
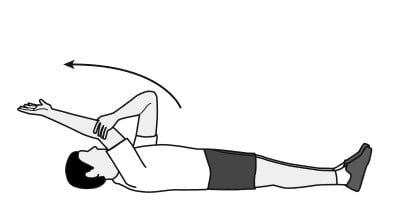
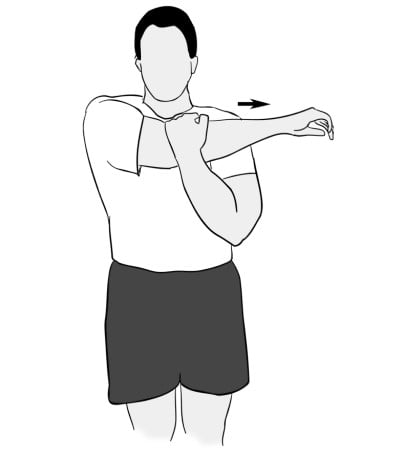
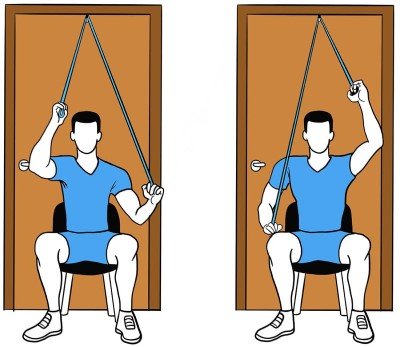
With the normal hand supporting the affected one, the shoulder is lifted up gradually in a position of flexion, abduction, and external rotation.
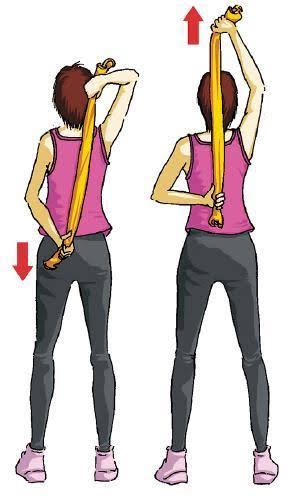
Here the patient carries the affected arm backward with the shoulder in a position of extension, adduction, and internal rotation with the elbow in 90 degrees flexion.




Preventive Measures:
For early detection of frozen shoulder, these simple tests may be helpful:
- In the supine position, the patient’s shoulder is passively adducted in elevation. If the patient complains of pain or stiffness in its terminal range, such a patient has more chances of developing periarthritis.
- In this, the patient’s position is side-lying. If there is pain, then there are more chances for future frozen shoulders.
- Certain patients such as diabetics, with fractures of the clavicle, shoulder, humerus, colles’ fracture, etc have a high risk of developing frozen shoulder. Also, patients with ischemic heart disease, respiratory diseases, etc, have a higher incidence of developing frozen shoulder.
- A positive apprehension test also indicated an impending frozen shoulder.
In all such patients, shoulder joint mobilization in the early stages is helpful to prevent future occurrence of frozen shoulder.
Conclusion:
Frozen shoulder is a very common condition nowadays. Physiotherapy treatment plays a very effective role in treating this condition. Along with this, frozen shoulder exercises are also helpful for a faster recovery.
BEST OF LUCK!